Neuroplasticity is the ability of the brain to form and reorganize synaptic connections, especially in response to learning or experience or following injury.
by Lisa Kreber, PhD CBIS
Neuroplasticity has been described as, "The science of how the brain changes its structure and function in response to input." With that, there are two important aspects of this definition. First, the brain really can change in relation to structure and function, unlike virtually any other organ of the body, such as the heart or liver. Specifically, it is designed to grow new structures and create new pathways in the presence of damage or an environmental challenge. Second, the phrase "in response to input," speaks directly to the fact that the brain doesn't really change unless you challenge it. Any task that is familiar, automatic, or easy does not challenge your brain, but activities that are difficult and challenging for your brain elicit changes in the neural network.
Dr. Donald Hebb, a Canadian neuropsychologist, famously stated, "Neurons that fire together, wire together." This means that neurons that communicate with each other end up being part of the same neural network and want to continue to communicate with each other. Repetition can be important in affecting this process.
It is important to point out that neuroplasticity or simply, plasticity, is not an occasional state in the nervous system, it is a normally ongoing state. This is because the brain in is designed to change in response to changes in the environment and not just through injury recovery. As neurologist Dr. David Perlmutter noted, "Neuroplasticity provides us with a brain that can adapt not only to changes inflicted by damage, but allows adaptation to any and all experiences and changes we may encounter." These changes occur in the anatomy through input to the neural system, as well as through output. In the treatment environment, this input occurs along afferent connections (from the periphery to the central nervous system), for example, with challenges to the brain through rehabilitation activities and learning a new skill. In turn, outputs from the brain to efferent targets (from the brain to the periphery) are manifested in ways that help us, as clinicians, measure progress, eg, how fast and accurately is a patient able to do a task?
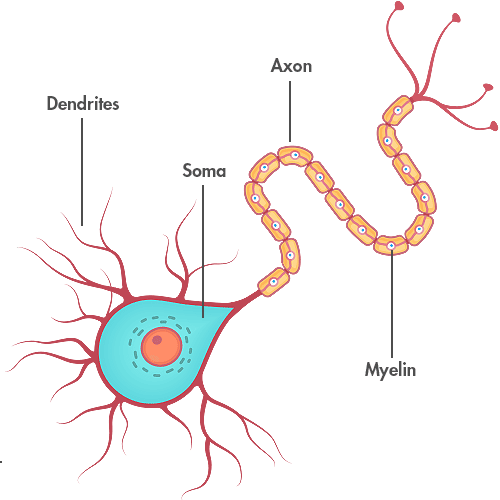
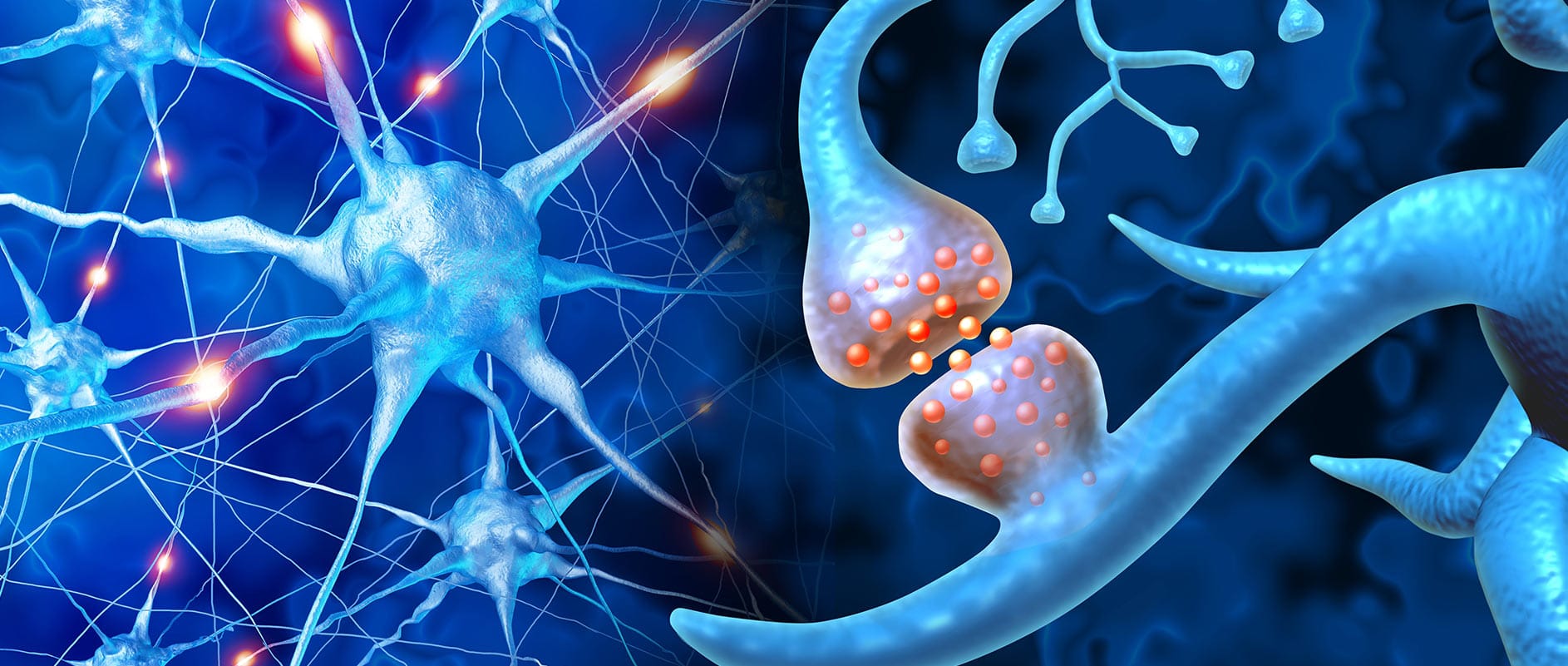
The process of normal neuronal firing takes place as a communication between neurons through electrical impulses and neurotransmitters. To better understand this process, it is important to understand the parts of a neuron, including the soma, dendrites, and axons. The soma can be thought of as the "brain" of the brain cell, as it processes the input/information into the cell and determines if it is important enough to pass along to another cell. The dendrites are tree-like structures that receive and gather information from other neurons for delivery to the soma, where the information is processed and, as mentioned, the determination is made whether it is important enough to pass along to other neurons. Such information is passed from neuron to neuron via the axons, which act like the cables or wires in your house. In addition, axons are insulated—similar to electrical wires—with a fatty substance called myelin to keep the electrical current strong and flowing in the right direction.
Abnormal neuronal firing can occur when the signals between neurons are somehow disrupted. Such a problem commonly occurs in the presence of axonal shearing as the structure and connection of the axon with cell body is disrupted or sheared from the cell body by trauma forces. This creates damage to the axons so that they are no longer able to communicate with neurons and the connection is lost, causing information to get stuck as it cannot be effectively passed on. Because of this, a neuron that is no longer able to receive input from lost connections will likely end up dying, unless it is able to establish a new connection with another neuron. Symptoms of diffuse axonal injury, or DAI, in a patient may manifest clinically in slow speed of processing, or for example, requiring increased time to hear what is being said, such as question, process that information, formulate a response and then, articulate that response.
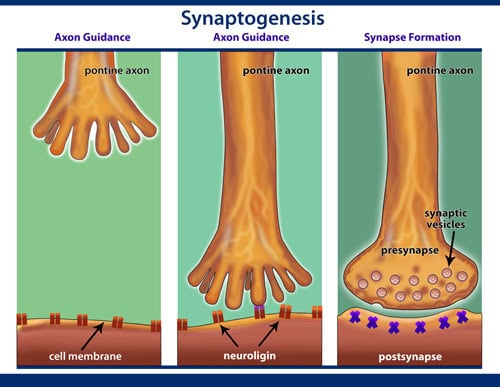
Neuroplasticity can be seen as the process of rebuilding the bridge between disconnected neurons and rehabilitation as a driving force in this process for providing the right input at the right time with the right amount of intensity to make these new connections. Inside the brain, this can occur through four major processes: angiogenesis, synaptogenesis, dendritic arborization, and neurogenesis. Angiogenesis is the creation of new blood vessels within brain structures. After a brain injury, there can be decreased blood flow to those structures when they can be most in need of more oxygen and glucose for recovery. From a rehabilitation standpoint, it has been determined that one of the best ways to induce angiogenesis is though physical exercise, especially aerobic exercise. Synaptogenesis is the creation of new synapses within brain structures and, similar to the effect of physical exercise on angiogenesis, cognitive exercise is what is needed to stimulate synaptic growth following an injury. Cognitive exercise also serves to stimulate dendritic arborization, which, as the name suggests, is the growth of dendritic spines similar to the branches of a tree, which serve to gather information from other neurons and from which additional dendrites can grow for the purpose of gathering still more information.
Finally, although there is some dispute as to whether or not the brain can actually "grow" completely new neurons or neurogenesis, it is the author's belief that although there are certain areas of the brain that actually grow new cells, in general, it is more likely that the majority of neuroplastic recovery is through the growth of new connections. The downside of the growth of new connections is the creation of maladaptive connections within the brain that are detrimental to recovery, such as in the case of seizure activity. What can be seen as perhaps the opposite of this is what the author has termed facilitated adaptive plasticity (FAP). This is the essence of the rehabilitation process, as therapy professionals in the treatment environment assist the patient to make the "right" neural connections.
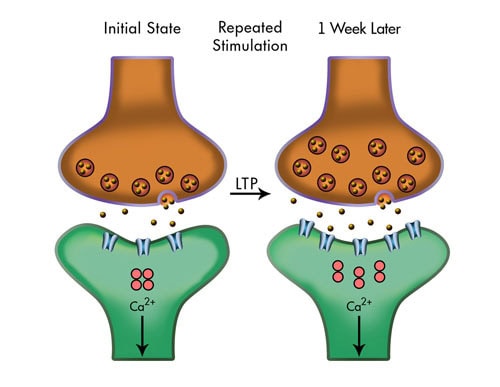
Plasticity can occur through processes that take time, known as slow-onset changes, or through quicker processes, known as fast-onset changes. Slow-onset changes are the anatomic changes of the neurons, including axonal growth, dendritic sprouting, and neurogenesis–growing completely new structures, while fast-onset changes are the activities that occur at the synaptic level. These kinds of fast-onset changes are known as synaptic modulation, which really means the ongoing process of strengthening or weakening of existing synapses. This process can be thought of much like the operation of your car, with the gas pedal representing excitation of synapses and the brake representing inhibition of synaptic responses. Thus, you really have two ways to make the brain go faster: strengthening synaptic connections through excitation (gas) and inhibition of other synaptic connections (brake). Persistent strengthening of synaptic connections through excitation (putting on the gas) develops long-term potentiation (LTP), or increasing the potential for that response to occur, while persistent weakening of other connections (putting on the brake) produces long-term depression (LTD) of a synaptic response.
During the course of human development, synapses are constantly formed and eliminated depending on whether or not specific neural connections are being utilized. This is where we get the "use it or lose it" idea. Through our early years of development, we actually have more connections than we need, so our brains go through a process of pruning or eliminating connections that are not being used. In women, this process generally occurs beginning in puberty, while in men this typically occurs in the early 20s. Throughout the lifespan after this pruning period, we continue to undergo the process of maintenance of available synapses, involving both axons and dendrites; a process which require a longer period of time. In addition, longer connections may not be able to regrow in older neural systems, but may be able to do so in younger brains with excess connectivity prior to the pruning period. Reactive synaptogenesis is a process which occurs quickly—within 10-15 minutes and occurs only during a learning task and may not lay down a lasting connection, whereas, as noted earlier, neurogenesis is a much slower process and requires growing an entirely new neuron. But exactly how can this be done?
Most people have heard about stem cells and their possible use with growing all kinds of new structures in the body, including growing new neurons. But what is less known is that there are really two types of stem cells. Pluripotent stem cells are what most people are familiar with. These are the types of cells that can be utilized to grow into virtually any type of cell in the body. The other type of stem cells are known as multipotent cells. These are stem cells that can become only certain types of cells in a specific category, such as those that can become different types of cells in the blood, such as monocytes, lymphocytes, or neutrophils. But, they cannot become anything other than a type of blood cell. One of the greatest challenges facing the field of stem cell research is in relation to the possibility of identifying and activating the correct type of multipotent stem cells for their designated use, including the correct cells that can become specific types of brain cells. Some of the things that we do know about stem cells in the brain are where they are created and replenished. One of these areas is known as the subventricular zone, just adjacent to the ventricles. Another area of stem cell production is in the olfactory bulb.
As this is the area which controls the sense of smell, it is thought that more cell replenishment might be needed in this area because the cells in this area might die at a higher rate than other brain cells. This is also related to why we lose our acuity of smell as we grow older, when these cells are not replenished with the frequency and volume of our youth. Still another area of stem cell production is in the subgranular zone/dentate gyrus of the hippocampus. This area is heavily involved with memory functions, and as you might suppose, requires frequent replenishment as you add more memories.
Because all of us are capable of producing our own stem cells, the ultimate possibility of being able, in the future, to use our own stem cells would virtually negate the current political and religious controversy regarding the acquisition and use of stem cells from others, if a way can be found to turn our own stem cells on or off as we need them.
As discussed earlier, modulation of synaptic activity occurs in the form of potentiation, an increase in the synaptic responsivity (excitability/sensitivity) of one cell communicating with another, or inhibition, the reduction of synaptic activity between one cell and another. In the spectrum of potentiation, posttetanic potentiation (PTP) is the shortest-lived event, lasting only a minute or two. Short-term potentiation (STP) lasts somewhat longer than PTP. Ultimately, long-term potentiation (LTP) lasts quite a bit longer and may actually change the physical structure of the synaptic connection. On the other end of the spectrum, long-term depression (LTD) is the inhibitory counterpart of long-term potentiation. This process is important as it is believed that while LTP is the mechanism through which memories are established, LTD may work to help us forget some things we don't really need so that the brain does not become overloaded attempting to remember everything. This is also related to the difference in how the brain creates short-term as opposed to long-term memories. Everything that is needed to establish and store short-term memories is already in synaptic abundance: proteins, receptors, ion channels, enzymes, and transporters, but only for a short time. Long-term memories are dependent on creating something–synthesizing new proteins or increasing the synthesis of already-existing proteins.
Unmasking is a process that changes the excitability or inhibition through an external process. An example of this is transcranial magnetic stimulation (TMS), which uses a magnetic field to either increase the excitability or inhibit a certain specific circuit in the brain. The idea behind this is essentially implementing an artificial way to get specific neurons to fire the way you want in an attempt to stimulate them to fire in this manner on their own.
There are two most characteristic forms of plasticity that occur within the brain in the presence of injury. The first is expansion of a specialized cortical area, such as may be seen in the case of someone who has suffered left hemiparesis after a stroke. They might be neglecting the left side altogether and begin using their right side for everything. This has the effect of reducing the cortical area for control of the left side, while expanding the cortical area controlling the right. This is why, especially in the context of treatment, it is important to continue to stimulate the left side cortical area so that cortical real estate doesn't go away. Another process of neuronal plasticity involves recruitment of a remote cortical area as a result of injury or new learning. An example of this could occur in the case of an individual who has experienced onset of blindness as a result of injury. In this situation, the occipital lobe, the area that processes vision, is no longer receiving input through the visual pathways and, in practicality, is no longer needed for that purpose. But as the person's other senses come to the forefront, such as a heightened sense of touch, this activity, to a certain degree, can be moved to the occipital lobe
From a treatment standpoint, methods of increasing neuroplasticity can include physical exercise, which has been found to increase neurotrophic factors, a kind of fertilizer for the brain, in addition to stimulating angiogenesis. Cognitive exercise can also increase a specific type of fertilizer called brain-derived neurotrophic factor (BDNF) and increases synaptogenesis. The question then arises, "What if these therapy activities were combined?" For example, what if you had someone walking on a treadmill while performing some type of cognitive activity so that you stimulate neurotrophic factors on two fronts? One study actually did find that such a combination of activities can exponentially enhance the production of neurotrophic factors.
Stress has been demonstrated to produce glucocorticoids, which are known as stress hormones, that can negatively impact our memory skills, as these stress hormones cause BDNF to decrease, especially in the hippocampus, the memory area. Have you ever been through a period where you feel really stressed out and just can't seem to remember even some simple things, like where we you left the keys or other things that should be simple and automatic? This may be why. In addition, continued release of these hormones over a period of time can decrease synaptic connectivity, and in the case of persons who are chronically stressed out, such as those who have PTSD, they may have trouble actually laying down new memories. Or possibly, the type of connectivity is changed, such that they seem to only retain the more negative memories regarding the events or situations that led to the PTSD. It is felt that these sorts of negative memories are the ones that become hard-wired and can be difficult to get rid of. In these situations, use of antidepressants may be effective.
Evidence also suggests that the brain produces increased trophic factors, especially BDNF, immediately following a brain injury; however, after a period of time, there is also a down-regulation of trophic factors, so earlier in the recovery process might be an important time to engage the patient, as much as possible, in physical and cognitive exercise to help get those trophic levels back up and to optimize recovery.
A common question from therapists and clinicians has to do with knowing what plasticity actually looks like in the treatment environment, the "How do I know if it really works?" question. While at times it can be hard to know, examples of plasticity at work might include the loss of previously acquired behaviors, such as a decrease in maladaptive behaviors or a decrease in seizures. Another example could be the release of normally suppressed behaviors, such as in the case of a patient with stroke increasing use of their affected side, or, as in the situation discussed earlier, of a person with adult-onset blindness. In this case, you might see the incomplete takeover of sensory function by a semi-adapted neighboring system. Finally, these changes might also manifest in the presence of new adaptive or maladaptive behaviors.
Kleim and Jones* outlined ten principles of neuroplasticity that can be helpful to keep in mind in the treatment environment:
"Use It or Lose It" "Neural circuits not actively engaged in task performance for an extended period of time begin to degrade." An example of this might be seen in the treatment of a patient who requires G-tube feeding due to an inability to be fed orally. Over time, the circuits responsible for the swallowing mechanism may actually begin to degrade due to lack of use. Subsequently, when that patient is able to begin to swallow again, they may require additional time and trials to reestablish this process as these circuits may be a bit rusty.
"Use It and Improve It" "Training that drives a specific brain function can lead to enhancement of that function." An example of this can be highlighted from the previous discussion of a patient with stroke who may have lost use of a particular side of their body and may be neglecting that side or not using it because it is simply too difficult. In the treatment setting, a technique known as constraint-induced movement therapy (CIMT) can be used to restrain the arm on the nonaffected side so that the patient is compelled to use their affected limb as much as possible and improve its function.
"Specificity" "The nature of the training experience dictates the nature of the plasticity." From a treatment standpoint, specificity highlights the importance of tailoring an activity or exercise to produce a result in specific circuitry. For example, as discussed earlier, physical exercise can be utilized to promote vascular growth, if that is your aim. By the same token, exercises and modalities geared toward enhancing swallowing might also be related to the circuitry involved in producing speech, but may not necessarily generalize to actually producing speech.
"Repetition Matters" "Induction of plasticity requires sufficient repetition." One of the challenges for therapists in the rehabilitation environment can often revolve around being able to quantify how much time or how many sessions of specific therapy a patient needs to recover certain skills. Stakeholders, especially insurance representatives and the patients themselves, want to know, "How long is it going to take to get better?" The truth is, we don't know these actual numbers, but we do know from research and study that thousands and tens of thousands of repetitions of certain activities are needed to generate these changes. Because of this, it may take utilizing techniques, such as combining therapies, to provide patients the opportunities for sufficient repetition of skills. For example, to get those thousands of steps that a patient may need to learn to walk again, a physical therapist may have the patient walking in and between their other therapies during the day or making sure they are getting up and out of their wheelchair when they are not in their PT session. By the same token, a physical therapist could help out the speech therapist by having the patient work on memory or path-finding activities during their PT session.
"Intensity Matters" "Induction of plasticity requires sufficient intensity." The question of proper therapy intensity follows this concept of repetition as well: "What is the proper dosage of therapy necessary? "How many sessions?" How long should these sessions be?' Research has also shown us that the more intensive the therapy program, the more likely a person is to achieve results and the more likely these changes are to be maintained over time.
"Time Matters" "Different forms of plasticity occur at different times during recovery." This principle is based on the idea that after an injury, the brain really wants to recover, so it makes sense that the earlier you provide the opportunity for recovery through these neuroplastic changes, the better. This early vs. late approach is especially important to support the beginning treatment before maladaptive behaviors have a chance to spring up.
"Salience Matters" "The training experience must be sufficiently salient to induce plasticity." What the person takes away from the training experience and what it means to them can affect their recovery. It is important for the therapist to know what is important to the patient, as emotions can modulate the strength of training or, for example, something like memory consolidation. If the therapist can make the training or information salient and important to the patient, they can more easily remember skills or pieces of information that are important to them, as their brains are often already overwhelmed with input.
"Age Matters" "Training-induce plasticity occurs more readily in younger brains." As discussed earlier, younger brains are already more plastic and adaptable to change than older brains, which is important to keep in mind when working with older versus younger patients.
"Transference or Generalization" "Plasticity in response to one training experience can enhance acquisition of similar behaviors." In the training process, the therapist needs to have an eye toward how a particular skill or activity can be generalized or transferred to real-world activities, such as increased independence in the home environment.
"Interference" "Plasticity in response to one training experience can impede acquisition of similar behaviors." When patients are actually able to come in for neurological treatment and that treatment is delayed, they often come in with compensatory behaviors for skill deficits, having already learned a different way of compensating, but which may not be the best way. With this, some of the challenge to learning the best way to regain a skill may involve unlearning some of these previously acquired behaviors.
* Kleim & Jones (2008), Principles of Experience-Dependent Neural Plasticity: Implications for Rehabilitation After Brain Damage. Journal of Speech, Language and Hearing Sciences, 51, S225-239.
In summary, plasticity of the brain serves to support learning and, by utilizing these inherent capabilities, therapists and clinicians can enhance recovery from brain injury by applying knowledge of these principles of plasticity directly to treatment.
CNS Monthly Newsletter
The latest CNS updates, including events, company information, and patient care developments
The Inside View
Quarterly magazine focused on brain injury research, rehabilitation, and advancements shaping the field
Sign-up for one or both to stay connected with brain injury news and recovery