Traumatic brain injury (TBI) can profoundly impact cognitive, physical, and psychological functioning. Physical challenges may include difficulties with mobility, balance, coordination, fine motor skills, strength, and endurance. Cognitive impairments frequently affect language, communication, memory, information processing, and perception. Psychological changes, such as shifts in emotional regulation and difficulty adapting to new limitations, are also common among those with TBI.
Brain injuries can arise from various circumstances. Traumatic brain injuries often occur during accidents where the head impacts an object, making this one of the most common causes; however, similar deficits can result from other types of brain injuries caused by oxygen deprivation, poisoning, or infections.
Mild traumatic brain injury (MTBI) is typically marked by symptoms such as brief unconsciousness, memory loss surrounding the injury, mental confusion during the incident, or focal neurological impairments. In many cases, individuals may appear outwardly unaffected while experiencing persistent functional challenges. Some people develop long-term effects from MTBI, known as post-concussion syndrome (PCS), which can significantly alter cognition and personality.
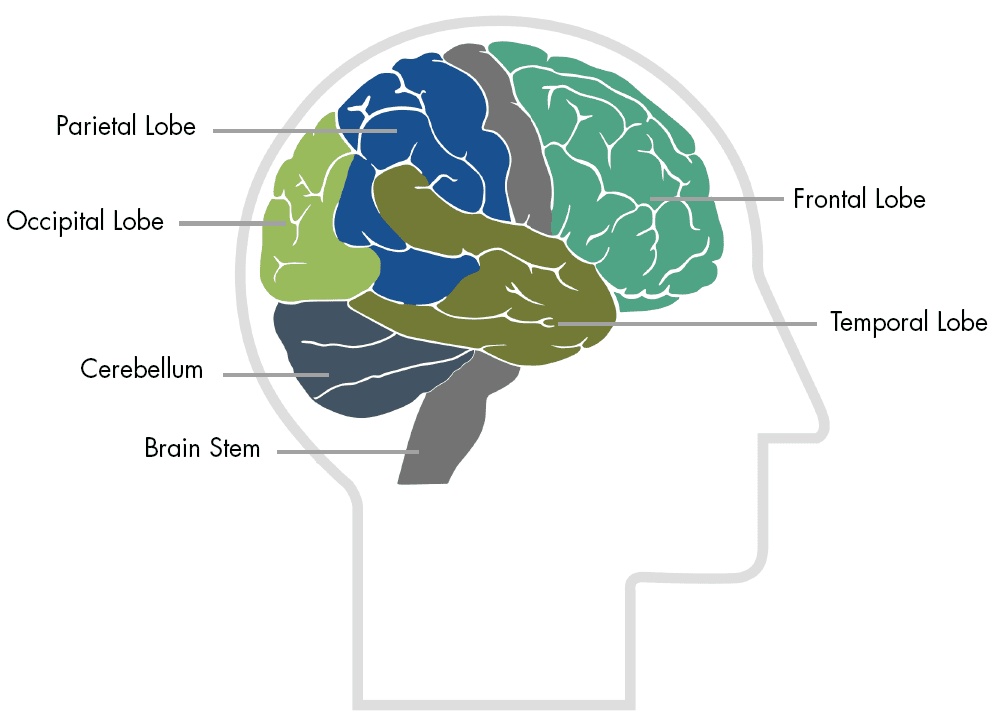
Most traumatic brain injuries involve widespread brain damage caused by the brain's movement within the skull during impact. This motion often results in diffuse axonal injury, where nerve cells become torn apart. Localized damage also occurs when the brain strikes the inner surface of the skull. Regions such as the brain stem, frontal lobe, and temporal lobe are particularly susceptible to damage due to their proximity to bony protrusions.
The brain stem, located at the brain's base, plays a critical role in regulating basic arousal, attention, and short-term memory. Injuries in this area can lead to confusion, frustration, and anger. Higher up in the brain, the limbic system regulates emotions and is connected to the temporal lobes, which are involved in memory and language. Damage to the temporal lobes or seizures originating from this region can contribute to behavioral disorders.
The frontal lobe, often injured due to its large size and location at the front of the cranium, governs cognitive functions and serves as the control center for emotions and personality. Damage here can lead to impaired judgment and heightened impulsivity, profoundly affecting an individual’s behavior and decision-making.
Traumatic brain injury can lead to a range of conditions that affect different aspects of health and well-being. These include:
Physical deficits: Challenges in ambulation, balance, coordination, fine motor skills, strength, and endurance
Cognitive deficits: Impairments in language, communication, information processing, memory, and perception
Psychological impacts: Alterations in emotional stability and difficulties in adjusting to disability
Injury mechanisms include direct impacts (eg, head striking an object) and nontraumatic causes like insufficient oxygen, poisoning, or infection.
Severe and mild TBI, including post-concussion syndrome, are among the spectrum of conditions associated with brain injuries.
Specific areas like the brain stem, frontal lobes, and temporal lobes are particularly vulnerable due to their proximity to bony structures.
Description
Specifically, anoxia is a condition in which there is an absence of oxygen supply to an organ's tissues although there is adequate blood flow to the tissue. Hypoxia is a condition in which there is a decrease of oxygen to the tissue in spite of adequate blood flow to the tissue. Anoxia and hypoxia, however, are often used interchangeably--without regard to their specific meanings--to describe a condition that occurs in an organ when there is a diminished supply of oxygen to the organ's tissues.
Anoxia and hypoxia may be caused by a number of events, such as smoke or carbon monoxide inhalation, high altitude exposure, strangulation, anesthetic accidents, or poisoning. In severe cases of anoxia and hypoxia, from any cause, the patient is often stuperous or comatose (in a state of unconsciousness) for periods ranging from hours to days, weeks, or months. Seizures, myoclonic jerks (muscle spasms or twitches), and neck stiffness may occur.
Treatment
Treatment of anoxia and hypoxia consists of establishing an adequate airway as soon as possible, using enough oxygen to saturate the blood, supporting the cardiovascular system as needed, and preventing or treating pneumonia. Respiratory assistance may be necessary.
Prognosis
If the patient's respiratory and cardiovascular systems can be supported properly, recovery may occur, but depends upon the severity of injury. As recovery proceeds, a variety of psychological and neurological abnormalities may appear, persist for a time, and then disappear. Mental changes such as dementia or a psychosis may occur. Mental confusion, personality regression, parietal lobe syndromes, amnesia, hallucinations, and memory loss may also occur.
Conditions Associated with TBI
Traumatic brain injury can lead to a range of conditions that affect different aspects of health and well-being. These include:
Physical Deficits: Challenges in ambulation, balance, coordination, fine motor skills, strength, and endurance.
Cognitive Deficits: Impairments in language, communication, information processing, memory, and perception.
Psychological Impacts: Alterations in emotional stability and difficulties in adjusting to disability.
Injury mechanisms include direct impacts (e.g., head striking an object) and non-traumatic causes like insufficient oxygen, poisoning, or infection. Severe and mild TBI, including post-concussion syndrome, are among the spectrum of conditions associated with brain injuries. Specific areas like the brain stem, frontal lobes, and temporal lobes are particularly vulnerable due to their proximity to bony structures.
Research
The NINDS supports and conducts studies aimed at understanding neurological conditions that can damage the brain such as anoxia and hypoxia. The goals of these studies are to find ways to prevent and treat these conditions.
These articles, available from a medical library, are sources of in-depth information on anoxia and hypoxia:
Bradley, W, et al (eds). Neurology in Clinical Practice: Principles of Diagnosis and Management, vol. II, Butterworth-Heinemann, Boston, pp. 1343-1349 (1991).
Joynt, R (ed). Clinical Neurology, vol. 2, Chapter 17, J.B. Lippincott Co., Philadelphia, pp. 1-18 (1990).
Nyakas, C, Buwalda, B, and Luiten, P. "Hypoxia and Brain Development." Progress in Neurobiology, 49:1; 1-51 (May 1996).
National Institute of Neurological Disorders and Stroke
National Institutes of Health
Bethesda, MD 20892
Aphasia is a disorder that results from damage to portions of the brain that are responsible for language. For most people, these are areas on the left side (hemisphere) of the brain. Aphasia usually occurs suddenly, often as the result of a stroke or head injury, but it may also develop slowly, as in the case of a brain tumor, an infection, or dementia. The disorder impairs the expression and understanding of language as well as reading and writing. Aphasia may cooccur with speech disorders such as dysarthria or apraxia of speech, which also result from brain damage.
Who has aphasia?
Anyone can acquire aphasia, including children, but most people who have aphasia are middleaged or older. Men and women are equally affected. According to the National Aphasia Association, approximately 80,000 individuals acquire aphasia each year from strokes. About one million people in the United States currently have aphasia.
What causes aphasia?
Aphasia is caused by damage to one or more of the language areas of the brain. Many times, the cause of the brain injury is a stroke. A stroke occurs when blood is unable to reach a part of the brain. Brain cells die when they do not receive their normal supply of blood, which carries oxygen and important nutrients. Other causes of brain injury are severe blows to the head, brain tumors, brain infections, and other conditions that affect the brain.
What types of aphasia are there?
There are two broad categories of aphasia: fluent and non-fluent. Damage to the temporal lobe (the side portion) of the brain may result in a fluent aphasia called Wernicke’s aphasia (see figure). In most people, the damage occurs in the left temporal lobe, although it can result from damage to the right lobe as well. People with Wernicke’s aphasia may speak in long sentences that have no meaning, add unnecessary words, and even create made-up words. For example, someone with Wernicke’s aphasia may say, “You know that smoodle pinkered and that I want to get him round and take care of him like you want before.” As a result, it is often difficult to follow what the person is trying to say. People with Wernicke’s aphasia usually have great difficulty understanding speech, and they are often unaware of their mistakes. These individuals usually have no body weakness because their brain injury is not near the parts of the brain that control movement.
A type of non-fluent aphasia is Broca’s aphasia. People with Broca’s aphasia have damage to the frontal lobe of the brain. They frequently speak in short phrases that make sense but are produced with great effort. They often omit small words such as ”is,” ”and,” and ”the.” For example, a person with Broca’s aphasia may say, ”Walk dog,” meaning, ”I will take the dog for a walk,” or ”book book two table,” for ”There are two books on the table.” People with Broca’s aphasia typically understand the speech of others fairly well. Because of this, they are often aware of their difficulties and can become easily frustrated. People with Broca’s aphasia often have right-sided weakness or paralysis of the arm and leg because the frontal lobe is also important for motor movements.
Another type of non-fluent aphasia, global aphasia, results from damage to extensive portions of the language areas of the brain. Individuals with global aphasia have severe communication difficulties and may be extremely limited in their ability to speak or comprehend language.
There are other types of aphasia, each of which results from damage to different language areas in the brain. Some people may have difficulty repeating words and sentences even though they can speak and they understand the meaning of the word or sentence. Others may have difficulty naming objects even though they know what the object is and what it may be used for.
How is aphasia diagnosed?
Aphasia is usually first recognized by the physician who treats the person for his or her brain injury. Frequently this is a neurologist. The physician typically performs tests that require the person to follow commands, answer questions, name objects, and carry on a conversation. If the physician suspects aphasia, the patient is often referred to a speech-language pathologist, who performs a comprehensive examination of the person’s communication abilities. The examination includes the person’s ability to speak, express ideas, converse socially, understand language, read, and write, as well as the ability to swallow and to use alternative and augmentative communication.
Where can I get more information?
NIDCD maintains a directory of organizations that can answer questions and provide printed or electronic information on aphasia. Please see the list of organizations at www.nidcd.nih.gov/directory. National Institute on Deafness and Other Communication Disorders National Institutes of Health 31 Center Drive, MSC 2320 Bethesda, MD USA 20892-2320 E-mail: nidcdinfo@nidcd.nih.gov
What Are the Cognitive and Communication Problems That Result From Traumatic Brain Injury?
Cognitive and communication problems that result from traumatic brain injury vary from person to person. These problems depend on many factors which include an individual's personality, preinjury abilities, and the severity of the brain damage.
The effects of the brain damage are generally greatest immediately following the injury. However, some effects from traumatic brain injury may be misleading. The newly injured brain often suffers temporary damage from swelling and a form of "bruising" called contusions. These types of damage are usually not permanent and the functions of those areas of the brain return once the swelling or bruising goes away. Therefore, it is difficult to predict accurately the extent of long-term problems in the first weeks following traumatic brain injury.
Focal damage, however, may result in long-term, permanent difficulties. Improvements can occur as other areas of the brain learn to take over the function of the damaged areas. Children's brains are much more capable of this flexibility than are the brains of adults. For this reason, children who suffer brain trauma might progress better than adults with similar damage.
In moderate to severe injuries, the swelling may cause pressure on a lower part of the brain called the brainstem, which controls consciousness or wakefulness. Many individuals who suffer these types of injuries are in an unconscious state called a coma. A person in a coma may be completely unresponsive to any type of stimulation such as loud noises, pain, or smells. Others may move, make noise, or respond to pain but be unaware of their surroundings. These people are unable to communicate. Some people recover from a coma, becoming alert and able to communicate.
In conscious individuals, cognitive impairments often include having problems concentrating for varying periods of time, having trouble organizing thoughts, and becoming easily confused or forgetful. Some individuals will experience difficulty learning new information. Still others will be unable to interpret the actions of others and therefore have great problems in social situations. For these individuals, what they say or what they do is often inappropriate for the situation. Many will experience difficulty solving problems, making decisions, and planning. Judgment is often affected.
Language problems also vary. Problems often include word-finding difficulty, poor sentence formation, and lengthy and often faulty descriptions or explanations. These are to cover for a lack of understanding or inability to think of a word. For example, when asking for help finding a belt while dressing, an individual may ask for "the circular cow thing that I used yesterday and before." Many have difficulty understanding multiple meanings in jokes, sarcasm, and adages or figurative expressions such as, "A rolling stone gathers no moss" or "Take a flying leap." Individuals with traumatic brain injuries are often unaware of their errors and can become frustrated or angry and place the blame for communication difficulties on the person to whom they are speaking. Reading and writing abilities are often worse than those for speaking and understanding spoken words. Simple and complex mathematical abilities are often affected.
The speech produced by a person who has traumatic brain injury may be slow, slurred, and difficult or impossible to understand if the areas of the brain that control the muscles of the speech mechanism are damaged. This type of speech problem is called dysarthria. These individuals may also experience problems swallowing. This is called dysphagia. Others may have what is called apraxia of speech, a condition in which strength and coordination of the speech muscles are unimpaired but the individual experiences difficulty saying words correctly in a consistent way. For example, someone may repeatedly stumble on the word "tomorrow" when asked to repeat it, but then be able to say it in a statement such as, "I'll try to say it again tomorrow."
How Are Cognitive and Communication Problems Assessed?
The assessment of cognitive and communication problems is a continual, ongoing process that involves a number of professionals. Immediately following the injury, a neurologist (a physician who specializes in nervous system disorders) or another physician may conduct an informal, bedside evaluation of attention, memory, and the ability to understand and speak. Once the person's physical condition has stabilized, a speech-language pathologist may evaluate cognitive and communication skills, and a neuropsychologist may evaluate other cognitive and behavioral abilities. Occupational therapists also assess cognitive skills related to the individual's ability to perform "activities of daily living" (ADL) such as dressing or preparing meals. An audiologist should assess hearing. All assessments continue at frequent intervals during the rehabilitative process so that progress can be documented and treatment plans updated. The rehabilitative process may last for several months to a year.
How Are Cognitive and Communication Problems Treated?
The cognitive and communication problems of traumatic brain injury are best treated early, often beginning while the individual is still in the hospital. This early therapy will frequently center on increasing skills of alertness and attention. They will focus on improving orientation to person, place, time, and situation, and stimulating speech understanding. The therapist will provide oral-motor exercises in cases where the individual has speech and swallowing problems.
Longer term rehabilitation may be performed individually, in groups, or both, depending upon the needs of the individual. This therapy often occurs in a rehabilitation facility designed specifically for the treatment of individuals with traumatic brain injury. This type of setting allows for intensive therapy by speech-language pathologists, physical therapists, occupational therapists, and neuropsychologists at a time when the individual can best benefit from such intensive therapy. Other individuals may receive therapy at home by visiting therapists or on an outpatient basis at a hospital, medical center, or rehabilitation facility.
The goal of rehabilitation is to help the individual progress to the most independent level of functioning possible. For some, ability to express needs verbally in simple terms may be a goal. For others, the goal may be to express needs by pointing to pictures. For still others, the goal of therapy may be to improve the ability to define words or describe consequences of actions or events.
Therapy will focus on regaining lost skills as well as learning ways to compensate for abilities that have been permanently changed because of the brain injury. Most individuals respond best to programs tailored to their backgrounds and interests. The most effective therapy programs involve family members who can best provide this information. Computer-assisted programs have been successful with some individuals.
What Research Is Being Done for Cognitive and Communication Problems Caused by Traumatic Brain Injury?
Researchers are studying many issues related to the special cognitive and communication problems experienced by individuals who have traumatic brain injuries. Scientists are designing new evaluation tools to assess the special problems that children who have suffered traumatic brain injuries encounter. Because the brain of a child is vastly different from the brain of an adult, scientists are also examining the effects of various treatment methods that have been developed specifically for children. These new strategies include the use of computer programs. In addition, research is examining the effects of some medications on the recovery of speech, language, and cognitive abilities following traumatic brain injury.
National Institute on Deafness and Other Communication Disorders
National Institutes of Health
31 Center Drive, MSC 2320
Bethesda, MD USA 20892-2320
nih.gov/nidcd
Description
A coma is a profound or deep state of unconsciousness. The affected individual is alive but is not able to react or respond to life around him/her. Coma may occur as an expected progression or complication of an underlying illness, or as a result of an event such as head trauma. A persistent vegetative state, which sometimes follows a coma, refers to a condition in which individuals have lost cognitive neurological function and awareness of the environment but retain noncognitive function and a perserved sleep-wake cycle. It is sometimes described as when a person is technically alive, but his/her brain is dead. However, that description is not completely accurate. In persistent vegetative state the individual loses the higher cerebral powers of the brain, but the functions of the brainstem, such as respiration (breathing) and circulation, remain relatively intact. Spontaneous movements may occur and the eyes may open in response to external stimuli, but the patient does not speak or obey commands. Patients in a vegetative state may appear somewhat normal. They may occasionally grimace, cry, or laugh.
Treatment
Once the patient is out of immediate danger, although still in coma or vegetative state, the medical care team will concentrate on preventing infections and maintaining the patient's physical state as much as possible. Such maintenance includes preventing pneumonia and bed sores and providing balanced nutrition. Physical therapy may also be used to prevent contractures (permanent muscular contractions) and orthopedic deformities that would limit recovery for the patients who emerge from coma.
Prognosis
The outcome for coma and vegetative state depends on the cause and on the location, severity, and extent of neurological damage: outcomes range from recovery to death. People may emerge from a coma with a combination of physical, intellectual, and psychological difficulties that need special attention. Recovery usually occurs gradually, with patients acquiring more and more ability to respond. Some patients never progress beyond very basic responses, but many recover full awareness. Patients recovering from coma require close medical supervision. A coma rarely lasts more than 2 to 4 weeks. Some patients may regain a degree of awareness after vegetative state. Others may remain in a vegetative state for years or even decades. The most common cause of death for a person in a vegetative state is infection such as pneumonia.
Research
The NINDS supports research on neurological conditions such as coma and persistent vegetative state. This research is aimed at finding ways to prevent, treat, and cure these conditions.
These articles, available from a medical library, are sources of in-depth information on coma:
Plum, F. "Disturbances of Consciousness and Arousal." In Cecil Textbook of Medicine, 19th edition, W.B. Saunders Co., Philadelphia, pp. 2048-2063 (1992).
Harris, J, and Berger, J. "Clinical Approach to Stupor and Coma." Chapter 5 in Neurology in Clinical Practice, Vol. 1, Butterworth-Heinemann, Boston, pp. 43-63 (1991).
National Institute of Neurological Disorders and Stroke
National Institutes of Health
Bethesda, MD 20892
A blow or jolt to the head can disrupt the normal function of the brain. Doctors often call this type of brain injury a "concussion" or a "closed head injury." Doctors may describe these injuries as "mild" because concussions are usually not life threatening. Even so, the effects of a concussion can be serious.
After a concussion, some people lose consciousness or are "knocked out" for a short time, but not always - you can have a brain injury without losing consciousness. Some people are simply dazed or confused. Sometimes whiplash can cause a concussion.
Because the brain is very complex, every brain injury is different. Some symptoms may appear right away, while others may not show up for days or weeks after the concussion. Sometimes the injury makes it hard for people to recognize or to admit that they are having problems.
The signs of concussion can be subtle. Early on, problems may be missed by patients, family members, and doctors. People may look fine even though they're acting or feeling differently.
Because all brain injuries are different, so is recovery. Most people with mild injuries recover fully, but it can take time. Some symptoms can last for days, weeks, or longer.
In general, recovery is slower in older persons. Also, persons who have had a concussion in the past may find that it takes longer to recover from their current injury.
This brochure explains what can happen after a concussion, how to get better, and where to go for more information and help when needed.
Medical Help
People with a concussion need to be seen by a doctor. Most people with concussions are treated in an emergency department or a doctor's office. Some people must stay in the hospital overnight for further treatment.
Sometimes the doctors may do a CT scan of the brain or do other tests to help diagnose your injuries. Even if the brain injury doesn't show up on these tests, you may still have a concussion.
Your doctor will send you home with important instructions to follow. For example, your doctor may ask someone to wake you up every few hours during the first night and day after your injury.
Be sure to carefully follow all your doctor's instructions. If you are already taking any medicines - prescription, over-the-counter, or "natural remedies" - or if you are drinking alcohol or taking illicit drugs, tell your doctor. Also, talk with your doctor if you are taking "blood thinners" (anticoagulant drugs) or aspirin, because these drugs may increase your chances of complications. If it's all right with your doctor, you may take acetaminophen (for example, Tylenol®* or Panadol®*) for headache or neck pain.
*Use of trade names is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
Danger Signs - Adults
In rare cases, along with a concussion, a dangerous blood clot may form on the brain and crowd the brain against the skull. Contact your doctor or emergency department right away if, after a blow or jolt to the head, you have any of these danger signs:
The people checking on you should take you to an emergency department right away if you:
Danger Signs - Children
Take your child to the emergency department right away if the child has received a blow or jolt to the head and:
Although you should contact your child's doctor if your child vomits more than once or twice, vomiting is more common in younger children and is less likely to be an urgent sign of danger than it is in an adult.
Symptoms of Concussion
"I just don't feel like myself."
The type of brain injury called a concussion has many symptoms. These symptoms are usually temporary, but may last for days, weeks, or even longer. Generally, if you feel that "something is not quite right," or if you're "feeling foggy," you should talk with your doctor.
Here are some of the symptoms of a concussion:
Young Children
Although children can have the same symptoms of brain injury as adults, it is harder for young children to let others know how they are feeling. Call your child's doctor if your child seems to be getting worse or if you notice any of the following:
Older Adults
Older adults with a brain injury may have a higher risk of serious complications such as a blood clot on the brain. Headaches that get worse or an increase in confusion are signs of this complication. If these signs occur, see a doctor right away.
Getting Better
"Sometimes the best thing you can do is just rest and then try again later."
How fast people recover from brain injury varies from person to person. Although most people have a good recovery, how quickly they improve depends on many factors. These factors include how severe their concussion was, what part of the brain was injured, their age, and how healthy they were before the concussion.
Rest is very important after a concussion because it helps the brain to heal. You'll need to be patient because healing takes time. Return to your daily activities, such as work or school, at your own pace. As the days go by, you can expect to gradually feel better.
If you already had a medical problem at the time of your concussion, it may take longer for you to recover from your brain injury. Anxiety and depression may also make it harder to adjust to the symptoms of brain injury.
While you are healing, you should be very careful to avoid doing anything that could cause a blow or jolt to your head. On rare occasions, receiving another concussion before a brain injury has healed can be fatal.
Even after your brain injury has healed, you should protect yourself from having another concussion. People who have had repeated brain injuries, such as boxers or football players, may have serious problems later in life. These problems include difficulty with concentration and memory and sometimes with physical coordination.
Tips for Healing - Adults
Here are a few tips to help you get better:
Tips for Healing - Children
Parents and caretakers of children who have had a concussion can help them heal by:
Where to Get Help
"It was the first time in my life that I couldn't depend on myself."
There are many people who can help you and your family as you recover from your brain injury. You don't have to do it alone.
Show this brochure to your doctor or health care provider and talk with them about your concerns. Ask your doctor whether you need specialized treatment and about the availability of rehabilitation programs.
Your doctor may be able to help you find a health care provider who has special training in the treatment of concussion. Early treatment of symptoms by professionals who specialize in brain injury may speed recovery. Your doctor may refer you to a neurologist, neuropsychologist, neurosurgeon, or specialist in rehabilitation.
Keep talking with your doctor, family members, and loved ones about how you are feeling, both physically and emotionally. If you do not think you are getting better, tell your doctor. For more information, see Resources for Getting Help.
Help for Families and Caregivers
"My husband used to be so calm. But after his injury, he started to explode over the littlest things. He didn't even know that he had changed."
When someone close to you has a brain injury, it can be hard to know how best to help. They may say that they are "fine" but you can tell from how they are acting that something has changed.
If you notice that your family member or friend has symptoms of brain injury that are getting worse or are not getting better, talk to them and their doctor about getting help. They may also need help if you can answer YES to any of the following questions:
You might also want to talk with people who have experienced what you are going through. The Brain Injury Association can put you in contact with people who can help.
Resources for Getting Help
"I thought I was all alone, but I'm not. There are lots of people out there who understand what I've been through."
Several groups help people with brain injury and their families. They provide information and put people in touch with local resources, such as support groups, rehabilitation services, and a variety of health care professionals.
Among these groups, the Brain Injury Association of America (BIAA) has a national office that gathers scientific and educational information and works on a national level to help people with brain injury. In addition, 44 affiliated state Brain Injury Associations provide help locally.
You can reach the BIAA office by calling the toll-free BIAA National Help Line at 1-800-444-6443. You can also get information through the national BIAA Web site at www.biausa.org. Both the Help Line and the Web site can provide you with information about your closest state Brain Injury Association.
More information about brain injury is available through the Centers for Disease Control and Prevention (CDC) Web site at www.cdc.gov/ncipc/tbi.
For More Information
1. BIAA National Help Line: 1-800-444-6443
2. BIAA Web site: biausa.org
3. CDC Web site: cdc.gov/ncipc/tbi
Centers for Disease Control and Prevention
Acknowledgment
This article draws inspiration and insights from Charles N. (Nick) Simkins, a renowned trial lawyer specializing in traumatic brain injury, electric shock, and lightning strike cases. His advocacy for addressing sexual dysfunction after injury underscores the importance of compassion and comprehensive care. His original reflections emphasize the challenges and importance of breaking the silence surrounding this deeply personal issue. The following has been edited for length and clarity.
The Hidden Struggle
While conversations about personal issues like hemorrhoids or even toilet paper are increasingly open, sexual dysfunction following lightning strikes, electric shocks, or traumatic brain injuries remains shrouded in silence. Despite its prevalence in medical literature, physicians rarely ask about these issues, leaving patients to navigate the physical, emotional, and relational impacts on their own.
Sexual dysfunction can stem from chronic pain, brain or psychological injury, depression, medication side effects, and other challenges common among survivors of these injuries. This article aims to foster understanding, dispel shame, and provide a foundation for meaningful conversations and treatment.
Why It’s So Hard to Talk About
Even in a culture where sexuality is central to humor, media, and relationships, discussing problems like diminished libido or physical complications can feel daunting. Both patients and doctors may hesitate, perpetuating cycles of silence and misunderstanding. As attorney Charles N. Simkins reflects, his own initial reluctance to address this issue revealed how deeply ingrained these taboos are, even among professionals.
However, silence only compounds the frustration and isolation faced by those experiencing sexual dysfunction. Bridging the gap between the patient’s lived experience and the physician’s understanding is essential for healing.
Understanding the Problem
Complex Causes
Sexual function depends on intricate balances—emotion, timing, physical health, and environmental factors. Injuries that disrupt these balances can result in:
Physical changes (e.g., erectile dysfunction, reduced vaginal lubrication)
Psychological impacts (e.g., depression, PTSD, or altered self-image)
Medication side effects that diminish libido or sexual response
For couples, these changes can lead to misunderstandings, hurt feelings, and further strain. For example:
An injured partner might avoid intimacy due to embarrassment, triggering feelings of rejection in their spouse.
A loss of libido may cause the uninjured partner to assume their loved one no longer cares, creating a cycle of guilt, arguments, and further withdrawal.
The Psychological Aspect
Drawing on the psychological concept of "strokes" (units of recognition or emotional validation), it’s clear that injury often disrupts the ways couples connect and support each other. Without this balance, intimacy can falter. For instance, couples who once shared laughter over dinner or enjoyed dancing may find those interactions replaced by therapy appointments and stress.
Moving Toward Solutions
Why Sexual Health Matters
According to the World Health Organization, sexual health is integral to overall well-being, involving physical, emotional, intellectual, and social aspects. Healthy sexual relationships can:
Improve quality of life
Strengthen emotional bonds
Enhance physical health
Acknowledging and addressing sexual dysfunction is a crucial step in reclaiming these benefits after injury.
What Patients Can Do
Opening a conversation with a doctor can feel intimidating. To help, consider preparing a letter outlining:
Changes in sexual patterns since the injury
Current medications (and concerns about side effects)
Questions about treatment options or referrals to specialists
Providing this information upfront can "break the ice" and empower both patient and physician to explore solutions.
Medical Insights
Extensive research underscores the connections between brain injuries, other medical conditions, and sexual dysfunction. For example:
Neurological Changes: Damage to the brain’s frontal lobes or limbic system can alter libido, sexual behavior, or response.
Medication Side Effects: Antidepressants, antihypertensives, and other drugs commonly prescribed after injuries often affect sexual function.
Hormonal Disruptions: Brain trauma can impair pituitary function, causing hormonal imbalances that affect libido and arousal.
Emotional and Relational Factors: Depression, anxiety, or role changes within a partnership often exacerbate the physical challenges of sexual dysfunction.
Next Steps
Rehabilitation is not just about physical recovery—it’s about rebuilding lives. Addressing sexual dysfunction is part of that process. While it requires courage to acknowledge these issues, help is available. From hormone therapy and medications to counseling and physical aids, solutions exist to improve sexual health and intimacy.
If you’re struggling, don’t wait. Start the conversation today—with your partner, your doctor, or a specialist.
Sources
Simkins, C. N. Original reflections on sexual dysfunction after injury.
World Health Organization (WHO) reports on sexual health.
Lezak, M. D. Neuropsychological Assessment.
Rosenthal et al., Rehabilitation of the Adult and Child with Traumatic Brain Injury.
Adams et al., Principles of Neurology.
Additional clinical studies on sexual dysfunction and brain injury recovery.
Traumatic brain injuries (TBI) and cerebral vascular accidents (CVA) frequently result in visual dysfunctions that impact balance, spatial orientation, and coordination. Symptoms such as double vision, headaches, and visual fatigue often stem from disruptions in the visual system, even when no direct eye injury is present. Neuro-optometric rehabilitation addresses these issues through specialized therapies like lenses and prisms, helping patients regain independence and improve quality of life. These targeted approaches integrate seamlessly with broader rehabilitation efforts to support recovery.
Traumatic Brain Injury (TBI) affects millions of individuals each year, impacting their lives and the lives of their families in profound ways. Understanding the prevalence, causes, and outcomes of TBI is essential to raising awareness and supporting effective care and rehabilitation. Explore the latest statistics on TBI to learn more about its widespread impact and the ongoing need for compassionate, comprehensive care.
Dr. C. OBREJA
211, rue Robespierre, 93170 Bagnolet, France
Introduction
Traumatic brain injury (TBI) is the main cause of death for patients less than 45 (1). TBI biomechanics explores the mechanical phenomena that cause the initial cranio-cerebral lesions and thus represents the starting point for the overall understanding of the TBI pathophysiology. TBI is the consequence of the spatiotemporal pressure variations occuring inside the brain during head traumas. The spatial distribution of the pressure gradient (PG) is responsible for the tissue strains (compression, tensile, shear), the cerebral lesions' localisation and the consequent neurological signs (2). Beside skull's deformation caused by the contact loading and determining skull vibrations and/or fractures, current biomechanical theories concern two inertial phenomena: the linear acceleration and the rotational head movements. The first theory explains the superficial brain lesions. The second theory seems better explain the deep cerebral lesions and the concussion mechanism but is still controversed (3). Here is exposed a new biomechanical approach that can explain the deep cerebral lesions and the common neurological signs observed after human head traumas.
Traumatic brain lesions
Focal and diffuse cerebral lesions are currently described. The focal lesions, also called cerebral contusions, are haemorrhagical and are visible on frequently performed radiological exams as the X-ray computed tomography. The focal lesions are often located in the superficial brain structures, close from the skull, but sometimes deep cerebral hematomas occur. The focal lesions always coexist with different degrees of diffuse cerebral lesions, also called "diffuse axonal injury" (DAI). The DAI is concentrated in the deep cerebral regions and is not visible on the radiological exams. Meanwhile, in accordance with its severity, the DAI is mainly responsible of various degrees of consciousness disturbances and further clinical outcome (2). The clinical entity corresponding to the rather pathological sense of the DAI term is the brain concussion.
Current Theories
The linear acceleration theory was first evoked about one century ago. Relative movements and secondary impacts occur between the skull and the brain during a head impact. The pressure increases in the superficial cerebral structures below the impact zone, proportionally to the head linear acceleration (4). This theory explains the superficial cerebral lesions' occurrence. It cannot explain the preferential DAI localisation in the deep cerebral structures (8), neither the traumatic deep cerebral hematoma. It cannot axplain neither why the loss of consciousnes and the memory troubles are the most frequent clinic signs occuring after head trauma - despite the fact that the resposible cerebral structures are deeply located.
According to the rotational movements' theory evoked in 1943 by Holbourn (5), DAI and deep cerebral hematoma are caused by the tensile strains occuring between superficial and deep cerebral structures during the head circular movements. In a large series of experiments on primates, Thibault and Gennarelli particularly supported the role of the rotational movements in the DAI occurrence (6).
The consequences of the skull's vibrations are poorly understood. It is probable that the low-frequency skull vibrations (below 200 Hz) mainly cause deep cerebral lesions, while high-frequency vibrations have more consequences on the superficial cerebral structures (7).
In real life head trauma all these phenomena coexist. In the mean time, DAI and brain concussion also occured in pure linear accelerated experimental head trauma (5) even if under the current approach, the linear acceleration theory cannot explain how deep cerebral structures can be injured while superficial cerebral structures are respected.
Stereotactical Theory
The stereotactical approach considers the geometrical shape of the interface skull-brain, the close interactions between the two structures during their relative movements and the resultant pressure waves propagation.
The shape of the interface skull-brain is approximately spherical. The skull-brain relative movements, caused by the acceleration phenomena - linear or rotational - and by the skull vibrations, generate secondary pressure waves with an approximately spherical wave front. Because the brain tissue is isotrop on concentric plans, the wave propagation velocity toward the deep cerebral structures is spatially homogenous.
C = (E/r)0,5
C = wave propagation velocity; E = resilience; r = density
The spherical shape of the wave front is thus conserved. Its spoke and its surface progressively decrease. Despite attenuation phenomenon and according to the energy conservation law, the amplitude of the pressure waves, and thus the pressure gradient, progressively increases toward the deep cerebral structures. It will be maximal in the geometrical centre of the implied skull vault segment (figure 1), particularly if no significant energy consumption process occurs in the superficial cerebral structures before. If such a superficial cerebral contusion occur, a pressure wave "shadow cone" is delimited towards the deep cerebral structures and thus the stereotactical summation phenomena are partly perturbed.
In low or medium-energy impacts, the skull vibrations have a significant role by generating successive wave fronts. Cumulative effects related to the temporal summation phenomena thus add to the spatial (stereotactical) ones.
In high-energy impacts, the acceleration phenomena are predominant. Because of the skull fractures that often occur, the skull vibrations are perturbed and their stereotactical consequences reduced. In the mean time, the high acceleration effects diminish the relative importance of the skull vibrations' consequences.
Discussion and Conclusion
The stereotactical phenomena explain common neurological signs
The stereotactical phenomena explain why the initial and reversible loss of consciousness (IRLC) is the most common posttraumatic neurological sign, even if the involved structure - the ascendant reticulate matter (ARM) - is placed in the deep cerebral regions. It can also explain why, after the IRLC, most patients don't have any focal neurological deficit (motor, sensitive or visual) related to the superficial cerebral structures' lesions or functional impairement. The functional recovery is faster for the neuronal circuits with less infrastructure lesions and if the superficial lesions were more important than the deep ones, the recovery of the focal deficits would be longer than the recovery of the consciousness.
The stereotactical phenomena also explain the high incidence of the memory disturbances after a head trauma as the result of the periventricular neuronal circuits' functional impairment or lesions. At our best knowledge, this is the first theory to explain these clinical phenomena. The isolated functional impairment of the ARM could also be explained by the fact that the consisting neuronal fibres are less resistant because nonmyelinated. This argument is not applicable to the myelinated neuronal fibres whose functional impairment or lesions generate the frequent posttraumatic memory disturbances.
The stereotactical phenomena explain the deep cerebral lesions
The stereotactical approach can also explain the preferential localisation of the DAI in corona radiata, corpus callosum, fornix and upper brainstem (8). These anatomical regions correspond to geometrical centres of different skull vault segments. Deep traumatic cerebral hematomas can also be better understood as they occur close to the geometrical centre of the skull vault.
The stereotactical phenomena explain the importance of the contrecoup cerebral lesions
The stereotactical phenomena explain why the cerebral contrecoup lesions (CCL) are often more important than the direct lesions (DL). The bend spoke of the lateral skull segment is approximately equal to the bi-parietal skull diameter. According to the stereotactical theory the CCL are the consequence of the pressure waves' stereotactical summation toward the geometrical centre of the implied skull vault segment. Thus, up to a critical energy lateral impact, the CCL occur before the DL.
The stereotactical phenomena explain why the cerebral contusions (direct or contrecoup) are often located in the temporal and the frontal lobes. These cerebral regions correspond to small bend spoke segments of the skull and contain their geometrical centre - where maximal stereotactical summation occurs.
The stereotactical phenomena are supported by prviously reported experimental data
In older experiments Gurdjian noted significant differences between the DAI localisation after head impacts on primates and dogs. The primates' brains had predominant DAI in the upper brainstem while the dogs' DAI was concentrated in the lower brainstem regions (9). These differences are unexplained by the current biomechanical theories, but they can be easily understood according to the stereotactical approach by the difference between the shape of the animals' skull vaults and their geometrical centre localisation. According to the stereotactical approach, the DAI is concentrated in the geometrical centre of the skull vault and, as the primates' skull vault is more incurved, their geometrical centre is placed higher than the dogs' one.
Other stereotactical phenomena
The radiosurgery uses the stereotactical principle in order to avoid massive irradiation of the superficial structures when a deep cerebral lesion (tumour, malformation) has to be irradiated. The total irradiation doze, aimed to destroy the deep lesion, is spatially fractionated in many convergent beams. Thus, the superficial structures receive only small fractions of the total irradiation doze and are preserved.
Sounds are also pressure waves. Microphones with parabolic reflective surfaces and the concert halls' architecture use the stereotactical principle in acoustic applications.
Conclusion
The stereotactical phenomena can explain common posttraumatic neurological signs and cerebral lesions. Its complementarity with the other biomechanical theories could allow us to integrate the TBI biomechanics in a common concept in order to better understand the TBI pathophysiology and also related pathological entities like boxers' chronic encephalopathy or even Alzheimer's disease (10). Further experimental and especially human observational research in TBI biomechanics is needed.
References
McIntosh TK, Smith DH, Meaney DF, Kotapka MJ, Gennarelli TA, Graham DI. Neuropathological sequelae of traumatic brain injury: relationship to neurochemical and biomechanical mechanisms. Lab Invest 74: 315-42, 1996
Teasdale, G, Mathew, P. Mechanisms of cerebral concussion, contusion and other effects of head injury. In: Julian R. Youmans editor, Neurological surgery. 4th ed. New York: W B Saunders Co, p 1533-46, 1996.
McLean, AJ Brain injury without head impact? In: Bandak, A.F., Eppinger, R.H., Ommaya, A.K. editors, Traumatic brain injury: bioscience and mechanics. Larchmont, NY, Mary Ann Liebert Inc, p 45-9, 1996.
Nahum, AM, Smith, RW, Ward, CC. Intracranial pressure dynamics during head impact. Proc. 21st Stapp Car Crash Conference, SAE No. 770922 p 339-66, 1977.
Holbourn, AS. Mechanics of head injuries. Lancet 2: 438-41, 1943
Thibault, LE, Gennarelli, TA. Brain injury: an analysis of neural and neurovascular trauma in the nonhuman primate. 34th Annual proceedings of the Association for the Advancement of Automotive Medicine, Des Plaines, IL, p 337-51, 1990.
Willinger, R, Taleb, L, Kopp, C. Modal and temporal analysis of head mathematical models. In: Bandak, A.F., Eppinger, R.H., Ommaya, A.K. editors, Traumatic brain injury: bioscience and mechanics. Larchmont, NY, Mary Ann Liebert Inc. p. 265-76, 1996.
Blumbergs, PC, Scott, G, Manavis, J, Wainwright, H, Simpson, DA, McLean, AJ. Staining of amyloid precursor to study axonal damage in mild head injury. Lancet 344: 1055-6, 1994.
Gurdjian, ES. Recent advances in the study of the mechanism of impact injury of the head - a summary. Clin Neurosurg 19: 1-42, 1972.
van Duijn, CM, Tanja, TA, Haaxma R Head trauma and the risk of Alzheimer desease Am J Epidemiol 135: 775-782, 1992.
Over the past 10 years as a result of a paper authored by Dr. Brent Masel, CNS Executive Vice President of Medical Affairs and scientist, our view of traumatic brain injury has changed significantly.
A traumatic brain injury is no longer seen as a singular isolated event, rather, it is believed to be the beginning of a disease process. According to our founder, Dr. Mark Ashley, a traumatic brain injury is disease causative and disease accelerated. We at CNS and CNS-CREF are committed to finding a cure for that disease.
We do not believe the cure for TBI will entail making the individual the way they were prior to the injury. Rather, the analogy would be a car that is badly wrecked. Once repaired, it is not the way it was before–but it is functional. And we aim to restore those functions lost in a TBI.
We know that the cure will not be due to one individual solitary scientific discovery. Rather, the cure is an enormous jigsaw puzzle with thousands and thousands of pieces, and therefore, we will cure brain injury one piece at a time. Brain injury therapists and physicians have already found many of those pieces. We have cured many aspects of speech and swallowing issues, motor problems, cognitive and behavioral issues. We have stopped seizures.
But there is so much more to do; so many pieces of the puzzle to discover. At CNS, finding those pieces is an overarching focus of everything we do every day, every hour and every second. Our clinicians and scientists are committed to finding new ways to restore function. We are truly committed to finding the cure.
The severity of a TBI may range from “mild,” i.e., a brief change in mental status or consciousness, to “severe,” i.e., an extended period of unconsciousness or amnesia after the injury. TBI can cause a wide range of functional short- or long-term changes affecting thinking, sensation, language, or emotions.
TBI can also cause epilepsy and increase the risk for conditions such as Alzheimer’s disease, Parkinson’s disease, and other brain disorders that become more prevalent with age.1
About 75% of TBIs that occur each year are concussions or other forms of mild TBI.2
Repeated mild TBIs occurring over an extended period of time (i.e., months, years) can result in cumulative neurological and cognitive deficits. Repeated mild TBIs occurring within a short period of time (i.e., hours, days, or weeks) can be catastrophic or fatal.3
General Tips to Help Aid in Recovery
References
Source: Centers for Disease Control and Prevention
Approximately half of severely head-injured patients will need surgery to remove or repair hematomas (ruptured blood vessels) or contusions (bruised brain tissue). Disabilities resulting from a TBI depend upon the severity of the injury, the location of the injury, and the age and general health of the individual. Some common disabilities include problems with cognition (thinking, memory, and reasoning), sensory processing (sight, hearing, touch, taste, and smell), communication (expression and understanding), and behavior or mental health (depression, anxiety, personality changes, aggression, acting out, and social inappropriateness). More serious head injuries may result in stupor, an unresponsive state, but one in which an individual can be aroused briefly by a strong stimulus, such as sharp pain; coma, a state in which an individual is totally unconscious, unresponsive, unaware, and unarousable; vegetative state, in which an individual is unconscious and unaware of his or her surroundings, but continues to have a sleep-wake cycle and periods of alertness; and a persistent vegetative state (PVS), in which an individual stays in a vegetative state for more than a month.
Source: National Institute of Neurological Disorders and Stroke
CNS Monthly Newsletter
The latest CNS updates, including events, company information, and patient care developments
The Inside View
Quarterly magazine focused on brain injury research, rehabilitation, and advancements shaping the field
Sign-up for one or both to stay connected with brain injury news and recovery