Robert P. Lehr Jr., PhD
Professor Emeritus, Department of Anatomy, School of Medicine,
Southern Illinois University
In traumatic brain injury, the brain may be injured in a specific location or the injury may be diffused to many different parts of the brain. It is this indefinite nature of brain injury that makes treatment unique for each individual patient. In the past twenty years, a great deal has been learned about brain function, and we learn more every day. We can make guesses about the nature of the problems an individual may have from knowing the location of a lesion. Diagnostic procedures such as computed tomography (CT) scans and magnetic resonance imagings (MRIs) can also provide information about a brain injury. As rehabilitation specialists, we can also learn about an injury by observing the day-to-day activities of the patient. All the activities we perform each day, whether physical or mental, are directed by different parts of our brains. It is important that you become familiar with brain function to better understand how therapies created by rehabilitation professionals help people with brain injuries. In order for you to better understand how the rehabilitation process works, we will guide you through the different parts of the brain and indicate some of the functions and problems resulting from injury.
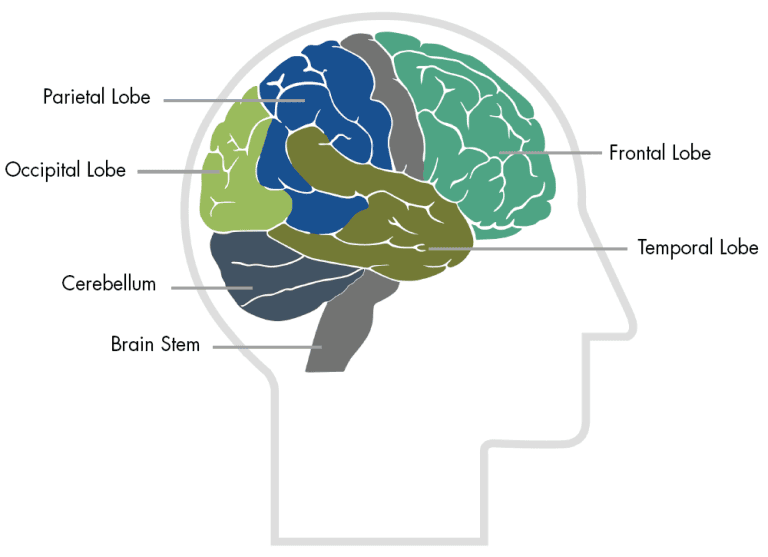
The brain has many parts, including the cerebral cortex, brainstem, and cerebellum. By listing some of the functions of each part of the brain, we will provide an overview of what problems occur after injury to these parts. It is important to understand that the brain functions as a whole by interrelating its component parts. The injury may only disrupt a particular step of an activity that occurs in a specific part of the brain. The interruption of that activity at any particular step, or out of sequence, can reveal the problems associated with the injury. Below is a list of functions and deficits or problems revealed when injury occurs at particular locations. The terms in parenthesis are the professional terms used to describe the deficit. Please refer to the Brain Map below of an illustration of the main areas of the brain.
Functions
Location for visual attention
Location for touch perception
Goal-directed voluntary movements
Manipulation of objects
Integration of different senses that allows for understanding a single concept
Observed Problems
Inability to attend to more than one object at a time
Inability to name an object (anomia)
Inability to locate the words for writing (agraphia)
Problems with reading (alexia)
Difficulty with drawing objects
Difficulty in distinguishing left from right
Difficulty with doing mathematics (dyscalculia)
Lack of awareness of certain body parts and/or surrounding space (apraxia) that leads to difficulties in self-care. Inability to focus visual attention
Difficulties with eye- and hand-coordination
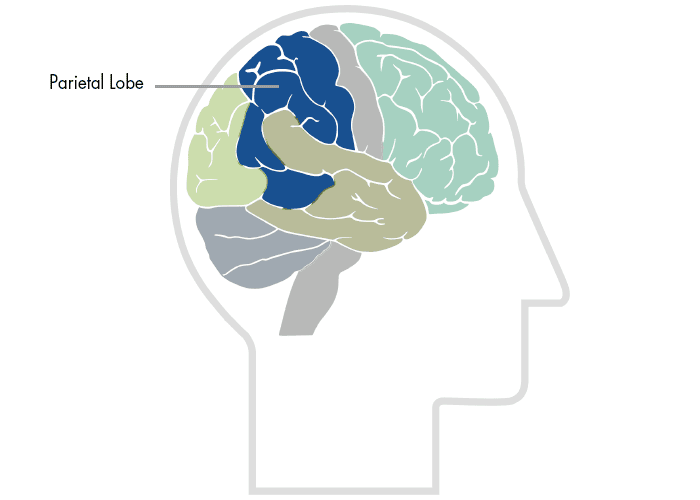
The parietal lobes can be divided into two functional regions. One involves sensation and perception and the other is concerned with integrating sensory input, primarily with the visual system. The first function integrates sensory information to form a single perception (cognition). The second function constructs a spatial coordinate system to represent the world around us. Individuals with damage to the parietal lobes often show striking deficits, such as abnormalities in body image and spatial relations (Kandel, Schwartz & Jessel, 1991).
Damage to the left parietal lobe can result in what is called "Gerstmann's Syndrome." It includes right-left confusion, difficulty with writing (agraphia) and difficulty with mathematics (acalculia). It can also produce disorders of language (aphasia) and the inability to perceive objects normally (agnosia).
Damage to the right parietal lobe can result in neglecting part of the body or space (contralateral neglect), which can impair many self-care skills such as dressing and washing. Right side damage can also cause difficulty in making things (constructional apraxia), denial of deficits (anosagnosia) and drawing ability.
Bi-lateral damage (large lesions to both sides) can cause "Balint's Syndrome," a visual attention and motor syndrome. This is characterized by the inability to voluntarily control the gaze (ocular apraxia), inability to integrate components of a visual scene (simultanagnosia), and the inability to accurately reach for an object with visual guidance (optic ataxia) (Westmoreland et al., 1994).
Special deficits (primarily to memory and personality) can occur if there is damage to the area between the parietal and temporal lobes.
Left parietal-temporal lesions can affect verbal memory and the ability to recall strings of digits (Warrington & Weiskrantz, 1977). The right parietal-temporal lobe is concerned with non-verbal memory.
Right parietal-temporal lesions can produce significant changes in personality.
Some common tests for parietal lobe function are: Kimura Box Test (apraxia) and the Two-Point Discrimination Test (somatosensory).
Kandel, J., Schwartz, J., & Jessell, T. Principles of Neural Science. 3rd edition. Elsevier. New York: NY, 1991.
Kimura, D. (1977). Acquisition of motor skill after left hemisphere damage. Brain, 100:527-542.
Warrington, E., & Weiskrantz, L. An analysis of short-term and long-term memory defects in man. In J.A. Deutsch, ed. The Physiological Basis of Memory. New York: Academic Press, 1973.
Westmoreland et al. Medical Neurosciences: An Approach to Anatomy, Pathology, and Physiology by Systems and Levels. Little, Brown and Company. New York: NY, 1994.
Functions
Observed Problems
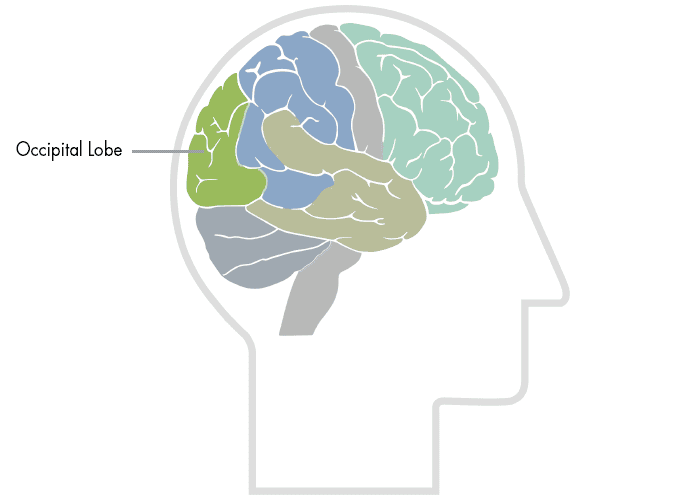
The occipital lobes are the center of our visual perception system. They are not particularly vulnerable to injury because of their location at the back of the brain, although any significant trauma to the brain could produce subtle changes to our visual-perceptual system, such as visual field defects and scotomas. The Peristriate region of the occipital lobe is involved in visuospatial processing, discrimination of movement and color discrimination (Westmoreland et al., 1994). Damage to one side of the occipital lobe causes homonomous loss of vision with exactly the same "field cut" in both eyes. Disorders of the occipital lobe can cause visual hallucinations and illusions. Visual hallucinations (visual images with no external stimuli) can be caused by lesions to the occipital region or temporal lobe seizures. Visual illusions (distorted perceptions) can take the form of objects appearing larger or smaller than they actually are, objects lacking color or objects having abnormal coloring. Lesions in the parietal-temporal-occipital association area can cause word blindness with writing impairments (alexia and agraphia) (Kandel, Schwartz & Jessell, 1991).
Kandel, E., Schwartz, J., & Jessell, T. Principles of Neural Science. 3rd edition. New York: NY. Elsevier, 1991.
Westmoreland, B. et al. Medical Neurosciences: An Approach to Anatomy, Pathology, and Physiology by Systems and Levels. New York: NY. Little, Brown and Compay, 1994.
Functions
Observed Problems
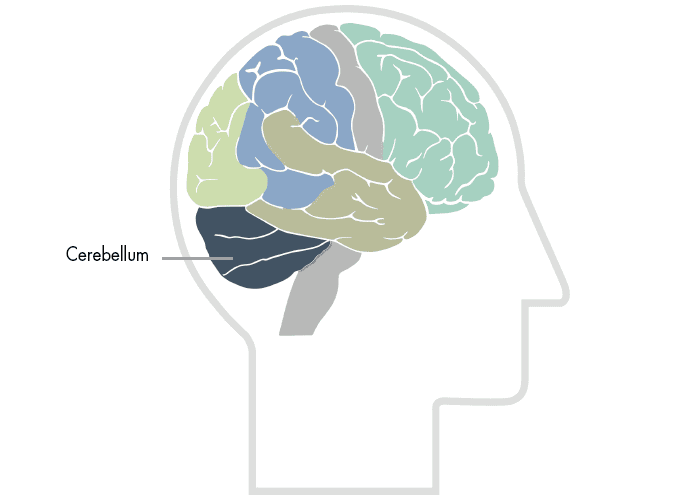
The cerebellum is involved in the coordination of voluntary motor movement, balance and equilibrium and muscle tone. It is located just above the brain stem and toward the back of the brain. It is relatively well protected from trauma compared to the frontal and temporal lobes and brain stem.
Cerebellar injury results in movements that are slow and uncoordinated. Individuals with cerebellar lesions tend to sway and stagger when walking.
Damage to the cerebellum can lead to: 1) loss of coordination of motor movement (asynergia), 2) the inability to judge distance and when to stop (dysmetria), 3) the inability to perform rapid alternating movements (adiadochokinesia), 4) movement tremors (intention tremor), 5) staggering, wide based walking (ataxic gait), 6) tendency toward falling, 7) weak muscles (hypotonia), 8) slurred speech (ataxic dysarthria), and 9) abnormal eye movements (nystagmus).
Functions
Breathing
Heart rate
Swallowing reflexes
Seeing and hearing (Startle response)
Controls sweating, blood pressure, digestion, and temperature (autonomic nervous system)
Affects level of alertness
Ability to sleep
Sense of balance (vestibular function)
Observed Problems
Decreased vital capacity in breathing, important for speech
Swallowing food and water (dysphagia)
Difficulty with organization/perception of the environment
Problems with balance and movement
Dizziness and nausea (vertigo)
Sleeping difficulties (insomnia, sleep apnea)

The brain stem plays a vital role in basic attention, arousal, and consciousness. All information to and from our body passes through the brain stem on the way to or from the brain. Like the frontal and temporal lobes, the brain stem is located in an area near bony protrusions making it vulnerable to damage during trauma.
Functions
How we know what we are doing within our environment (consciousness)
How we initiate activity in response to our environment
Judgments we make about what occurs in our daily activities
Controls our emotional response
Controls our expressive language
Assigns meaning to the words we choose
Involves word associations
Memory for habits and motor activities
Observed Problems
Loss of simple movement of various body parts (paralysis)
Inability to plan a sequence of complex movements needed to complete multi-stepped tasks, such as making coffee (sequencing)
Loss of spontaneity in interacting with others
Loss of flexibility in thinking
Persistence of a single thought (perseveration)
Inability to focus on task (attending)
Mood changes (emotionally labile)
Changes in social behavior
Changes in personality
Difficulty with problem solving
Inability to express language (Broca's aphasia)
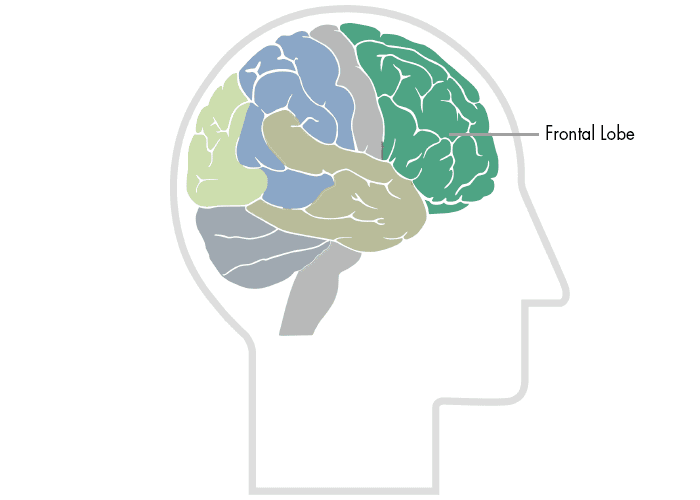
The frontal lobes are considered our emotional control center and home to our personality. There is no other part of the brain where lesions can cause such a wide variety of symptoms (Kolb & Wishaw, 1990). The frontal lobes are involved in motor function, problem solving, spontaneity, memory, language, initiation, judgement, impulse control, and social and sexual behavior. The frontal lobes are extremely vulnerable to injury due to their location at the front of the cranium, proximity to the sphenoid wing and their large size. MRI studies have shown that the frontal area is the most common region of injury following mild to moderate traumatic brain injury (Levin et al., 1987).
There are important asymmetrical differences in the frontal lobes. The left frontal lobe is involved in controlling language related movement, whereas the right frontal lobe plays a role in non-verbal abilities. Some researchers emphasize that this rule is not absolute and that with many people, both lobes are involved in nearly all behavior.
Disturbance of motor function is typically characterized by loss of fine movements and strength of the arms, hands and fingers (Kuypers, 1981). Complex chains of motor movement also seem to be controlled by the frontal lobes (Leonard et al., 1988). Patients with frontal lobe damage exhibit little spontaneous facial expression, which points to the role of the frontal lobes in facial expression (Kolb & Milner, 1981). Broca's Aphasia, or difficulty in speaking, has been associated with frontal damage by Brown (1972).
An interesting phenomenon of frontal lobe damage is the insignificant effect it can have on traditional IQ testing. Researchers believe that this may have to do with IQ tests typically assessing convergent rather than divergent thinking. Frontal lobe damage seems to have an impact on divergent thinking, or flexibility and problem solving ability. There is also evidence showing lingering interference with attention and memory even after good recovery from a TBI (Stuss et al., 1985).
Another area often associated with frontal damage is that of "behavioral sponteneity." Kolb & Milner (1981) found that individual with frontal damage displayed fewer spontaneous facial movements, spoke fewer words (left frontal lesions) or excessively (right frontal lesions).
One of the most common characteristics of frontal lobe damage is difficulty in interpreting feedback from the environment. Perseverating on a response (Milner, 1964), risk taking, and non-compliance with rules (Miller, 1985), and impaired associated learning (using external cues to help guide behavior) (Drewe, 1975) are a few examples of this type of deficit.
The frontal lobes are also thought to play a part in our spatial orientation, including our body's orientation in space (Semmes et al., 1963).
One of the most common effects of frontal damage can be a dramatic change in social behavior. A person's personality can undergo significant changes after an injury to the frontal lobes, especially when both lobes are involved. There are some differences in the left versus right frontal lobes in this area. Left frontal damage usually manifests as pseudodepression and right frontal damage as pseudopsychopathic (Blumer and Benson, 1975).
Sexual behavior can also be effected by frontal lesions. Orbital frontal damage can introduce abnormal sexual behavior, while dorolateral lesions may reduce sexual interest (Walker and Blummer, 1975).
Some common tests for frontal lobe function are: Wisconsin Card Sorting (response inhibition); Finger Tapping (motor skills); Token Test (language skills).
Blumer, D., & Benson, D. Personality changes with frontal and temporal lobe lesions. In D. Benson and D. Blumer, eds. Psychiatric Aspects of Neurologic Disease. New York: Grune & Stratton, 1975.
Brown, J. Aphasia, Apraxia and Agnosia. Springfield, IL: Charles C. Thomas, 1972.
Drewe, E. (1975). Go-no-go learning after frontal lobe lesion in humans. Cortex, 11:8-16.
Kolb, B., & Milner, B. (1981). Performance of complex arm and facial movements after focal brain lesions. Neuropsychologia, 19:505-514.
Kuypers, H. Anatomy of the descending pathways. In V. Brooks, ed. The Nervous System, Handbook of Physiology, vol. 2. Baltimore: Williams and Wilkins, 1981.
Leonard, G., Jones, L., & Milner, B. (1988). Residual impairment in handgrip strength after unilateral frontal-lobe lesions. Neuropsychologia, 26:555-564.
Levin et al. (1987). Magnetic resonance imaging and computerized tomography in relation to the neurobehavioral sequelae of mild and moderate head injuries. Journal of Neurosurgery, 66, 706-713.
Miller, L. (1985). Cognitive risk taking after frontal or temporal lobectomy. I. The synthesis of fragmented visual information. Neuropsychologia, 23:359-369.
Milner, B. Some effects of frontal lobectomy in man. In J. Warren and K. Akert, eds. The Frontal Granular Cortex and Behavior. New York: McGraw-Hill, 1964.
Semmes, J., Weinstein, S., Ghent, L., & Teuber, H. (1963). Impaired orientation in personal and extrapersonal space. Brain, 86:747-772.
Stuss, D. et al. (1985). Subtle neuropsychological deficits in patients with good recovery after closed head injury. Neurosurgery, 17, 41-47.
Walker, E., & Blumer, D. The localization of sex in the brain. In K.J. Zulch, O. Creutzfeldt, and G. Galbraith, eds. Cerebral Localization, Berlin and New York: Springer-Verlag, 1975.
Functions
Hearing ability
Memory acquisition
Some visual perceptions
Categorization of objects
Observed Problems
Difficulty in recognizing faces (prosopagnosia)
Difficulty in understanding spoken words (Wernicke's aphasia)
Disturbance with selective attention to what we see and hear
Difficulty with identification of, and verbalization about objects
Short-term memory loss
Interference with long-term memory
Increased or decreased interest in sexual behavior
Inability to categorize objects (categorization)
Right lobe damage can cause persistent talking
Increased aggressive behavior.
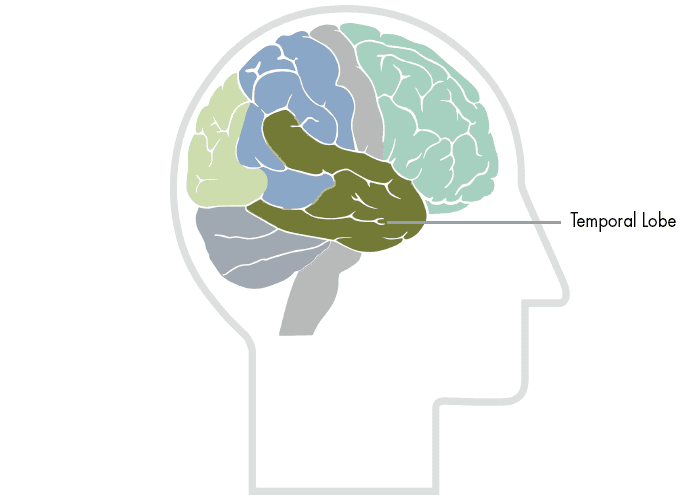
Kolb & Wishaw (1990) have identified eight principle symptoms of temporal lobe damage: 1) disturbance of auditory sensation and perception, 2) disturbance of selective attention of auditory and visual input, 3) disorders of visual perception, 4) impaired organization and categorization of verbal material, 5) disturbance of language comprehension, 6) impaired long-term memory, 7) altered personality and affective behavior, 8) altered sexual behavior.
Selective attention to visual or auditory input is common with damage to the temporal lobes (Milner, 1968). Left side lesions result in decreased recall of verbal and visual content, including speech perception. Right side lesions result in decreased recognition of tonal sequences and many musical abilities. Right side lesions can also affect recognition of visual content (e.g. recall of faces).
The temporal lobes are involved in the primary organization of sensory input (Read, 1981). Individuals with temporal lobes lesions have difficulty placing words or pictures into categories.
Language can be affected by temporal lobe damage. Left temporal lesions disturb recognition of words. Right temporal damage can cause a loss of inhibition of talking.
The temporal lobes are highly associated with memory skills. Left temporal lesions result in impaired memory for verbal material. Right side lesions result in recall of non-verbal material, such as music and drawings.
Seizures of the temporal lobe can have dramatic effects on an individual's personality. Temporal lobe epilepsy can cause perseverative speech, paranoia and aggressive rages (Blumer and Benson, 1975). Severe damage to the temporal lobes can also alter sexual behavior (e.g. increase in activity) (Blumer and Walker, 1975). Common tests for temporal lobe function are: Rey-Complex Figure (visual memory) and Wechsler Memory Scale - Revised (verbal memory).
Blumer, D., & Benson, D. Personality changes with frontal and temporal lesions. In D.F. Benson and F. Blumer, eds. Psychiatric Aspects of Neurologic Disease. New York: Grune & Stratton, 1975. Blumer, D., & Walker, E. The neural basis of sexual behavior. In D.F. Benson and F. Blumer, eds. Psychiatric Aspects of Neurologic Disease. New York: Grune & Stratton, 1975. Kolb, B., & Whishaw, I. (1990). Fundamentals of Human Neuropsychology. W.H. Freeman and Co., New York. Milner, B. (1968). Visual recognition and recall after right temporal lobe excision in man. Neuropsychologia, 6:191-209. Milner, B. (1975). Psychological aspects of focal epilepsy and its neurosurgical management. Advances in Neurology, 8:299-321. Read, D. (1981). Solving deductive-reasoning problems after unilateral temporal lobectomy. Brain and Language, 12:116-127. Taylor, L. (1969). Localization of cerebral lesions by psychological testing. Clinical Neurosurgery, 16:269-287.
Obtaining a general understanding of the brain and its functions is important to understanding the rehabilitation process. It is very important to understand that the rehabilitation professional is concerned with the whole person. The identification of individual problems gives the rehabilitation team areas in which to focus treatment plans. All of these plans are designed to work toward the rehabilitation of the whole person. Each problem area affects other areas and many times, resolving one problem has a major impact on other problems. For example, reestablishing postural balance and eliminating dizziness greatly enhances concentration and attention, which allows for improved cognition and problem solving.
CNS Monthly Newsletter
The latest CNS updates, including events, company information, and patient care developments
The Inside View
Quarterly magazine focused on brain injury research, rehabilitation, and advancements shaping the field
Sign-up for one or both to stay connected with brain injury news and recovery